Urinary tract infections (UTI’s) are common with approximately 2% of all children experiencing a UTI by 10 years of age . As uropathogenic bacteria ascend the urethra to gain access to the bladder it is not surprising that more girls than boys will get an infection. What is not generally recognized is that no matter the gender, the most common time to develop a UTI is in the first six months of life as the immune system is still developing. In countries where circumcision is not practiced, more boys than girls will get a UTI in infancy do to the retention of bacteria in the preputial space. No matter the age of the patient it is only urine infections that are associated with fever that are a threat to the kidney. Studies suggest that perhaps 10% of well treated patients with renal parenchymal involvement will develop a renal scar at long term assessment with sophisticated imaging. The import of such scars is debated but in general one may estimate that a scarred kidney is associated with a slightly higher life time risk of hypertension. Lacking fever, a UTI is not a threat to the kidney. In addition to fever, symptoms of UTI include dysuria, hematuria, urgency, incontinence, frequency and tummy pain. It needs be stated that each of these symptoms can be present in children in the absence of urine infection. This truism underscores the need to diagnose UTI on the basis of a urine culture and sensitivity. Recognize, however, that standard culture results are reported in bacterial colonies/cc of urine; these results do not absolutely confirm the occurrence of an infection, but suggest only on a statistical basis that a clinically significant infection is present. Proper interpretation must account for the method of urine collection ie bagged, catheter obtained, or voided with mid stream collection. While dipstick testing can suggest the possibility of UTI, urine culture is necessary to confirm the clinical impression. While more children get a UTI in the first year of life than any other time, another peak in occurrence is around the age of potty training. As the bladder expands its capacity, there is a longer time between voids which allows a longer time for any bacteria present to multiply and result in a clinical infection. Voiding cystourethrography (VCUG) was developed in the 1960’s and allowed for the diagnosis of vesicoureteral reflux (VUR). This retrograde flow of urine backward toward the kidney is present in 30% of children with UTI, no matter whether associated with fever or lower tract symptoms. VUR is also associated with the observation of scarred kidneys and for many decades Pediatric Urology believed the paradigm that VUR caused the renal scarring when associated with UTI and renal integrity could be protected by surgically correcting the VUR. It is now understood that many damaged kidneys associated with refluxing ureters (particularly the higher grades of VUR) are congenitally abnormal quite separate from any effects of infection on the kidney. As many children outgrow VUR another well established Pediatric Urologic practice has been to place children on continuous antibiotic prophylaxis (CAP) to protect the kidneys from harm while the VUR resolves. Recent high quality studies question the benefit of CAP and most clinicians are now very aware of the possible harm, individual and societal, from the overuse of antibiotics. Accepting that CAP may not be prudent, many question the need for obtaining VCUG’s. Additionally, in the United Kingdom, expert boards (NICE guidelines) have suggested that surgery for most VUR is not necessary. It is absolutely true that the rate of pediatric chronic kidney disease (CKD)has not changed in an era when VUR was treated aggressively with surgery. In Italy, a population based study of all children with CKD showed that 30% had VUR. However the CKD could be predicted in infancy because of the congenital dysplasia seen in the kidneys with reflux on renal sonography. No child who started out with normal kidneys and VUR ended up with CKD because of recurrent febrile UTI’s. While it is true that surgical correction of VUR decreases the rate of febrile UTI (fUTI), no study has shown that the rate of new renal scarring is decreased by surgical intervention. The above observations have attenuated the desire to diagnose VUR, recommend CAP for management or intervene surgically to correct the VUR. To underscore the current confusion a recent review of CPT coding at 90 US academic medical centers showed that for some surgeons, 90% of the patients with the diagnosis of VUR had surgical correction but for other surgeons less than 5% of the patients with this diagnosis had operative intervention. Presumably at these academic institutions all patients were managed with a good renal outcome. In any event, the most recent American Academy of Pediatric Guidelines for UTI (2011) take all of the above into account and recommend that catheterized specimens be used to obtain urine cultures in infants between 2 months and 2 years of age. Additionally the AAP recommends only a Renal and Bladder ultrasound for children with a fUTI. The VCUG is reserved for those children with abnormalities on the RBUS.
While the discourse continues, it is clear that beyond the age of potty training, most UTI’s occur for identifiable reasons and those reason most commonly have to do with bladder and bowel dysfunction (BBD). It is also clear that the UTI’s will be recurrent until the underlying causes are addressed. The physical exam is of primary importance in patients with UTI. The male exam is relatively straightforward and as noted above the circumcision status has relevance (though the UTI causing effect of the prepuce does decrease with age). In girls however it is very important to visualize the introitus, urethra and hymenal ring. The frog leg position is embarrassing, but necessary. Gentle outward traction on each labia should demonstrate the normal urethral and vaginal openings. Often urine will be seen pooling in the vagina and the secondary introital irritation is the obvious cause of the UTI. We don’t care much for wiping in either direction, but we do instruct the little girls to spread their labia and “Squat and Blot” to be rid of this vaginally retained urine. Obvious labial fusion can result from this vaginal retention of urine and , trapped urine has no egress causing UTI’s. In both boys and girls the inspection of the underwear is as important as the genitalia. Many, many patients who absolutely have no problems with wetting or their bowel habit are seen to be both wet and soiled on their underwear. The parents don’t appreciate the wet underwear as anything more than “leakage” and the soiling is felt to be a normal result of passing flatus in children. Palpating the abdomen often discloses stool in the left lower quadrant. One of the great problems in managing BBD in these patients is that the parents are globally unaware of the bowel habits of their children. Once the children are out of diapers, they really are on their own. We find ourselves having to convince the families that their child’s bowel habit is not normal. We think in terms of P5; that is Poorly Perceived Parental Perception of Pooping. While many rely on the KUB x-ray to demonstrate the fecal burden to the parents, we have developed the BMI (Bowel Movement Index). We use the renal and bladder ultrasound to image both kidneys and bladder for obvious benefit, but the bladder also provides a good acoustic window for stool in the rectum. We measure the stool in two dimensions sonographically and with multiplication derive a number; our BMI or area of the stool. It is useful to show the parents the lump of stool allowing awareness that their child, though they may have a BM a day, does not completely evacuate and that the retained stool which pushes on the bladder to cause the wetting. To sort out the wetting and soiling we rely on the voiding diary recording how often the patient voids and how much urine is produced with each void. Additionally the Bristol Stool Scale is very useful in getting the families in tune with their child bowel habits and how the bowel adversely affects the bladder. Once we get the family to understand that their
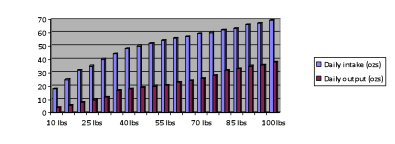
child’s urologic problems derive from the universally present constipation we can start improving things; clearly our #1 is the patient’s #2! While Miralax is likely the most common prescription given in Pediatric Urology offices nationwide, but we prefer to recommend nutritional management instead . The real challenge is to get the family to embrace the behavioral and dietary changes that are necessary to experience improvement. As a nation we are addicted to calorie dense, low fiber , fast, packaged and processed foods. None of which benefit colonic well being. We advocate a diet of real foods….avoid anything that comes in a package. It is a struggle as change is hard for many families to accept. For the typical child who wets because of the retained stool burden pushing on the bladder a tension develops. Clearly increasing fluid intake is the cornerstone of management for constipation, but just as clearly forcing fluids mandates that the bladder process more urine than the child chooses to deal with. Limiting fluids therefore benefits the bladder, but can worsen the bowel habit. Below is a useful chart showing the fluid requirement in ozs as well as the urine output in ozs for children of varying weights. In our management of children who wet, we often find that the children are over hydrated.
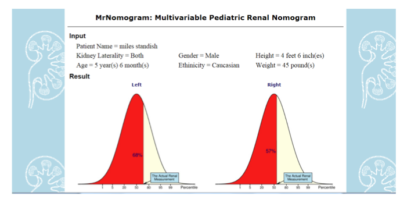
In managing children with BBD and UTI’s it is useful to know that they have normal sized kidneys. Our renal nomogram , found at https://www.prevmed.sunysb.edu/jjc/MrNomo is useful in generating a graphic depiction of the patient’s kidney size compared to normal. Below is a typical printable graphic obtained for a hypothetical patient.
Another site that may be useful for parents of children with BBD with or without UTI is
www.bladderandboweldysfunction.com